Asthma Prevalence
• Overall, an estimated 6% of children (or 173,000 children) in the county had asthma in 1999-2000.
• The prevalence of asthma was 7% among males and 5% among females.
• Asthma prevalence was 7% among children 6 to 17 years old and 5% among those 5 years of age and younger.
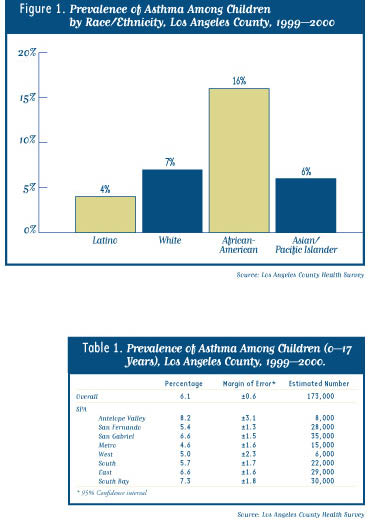
• The prevalence was more than two times higher among African-American children (16%) than white (7%), Asian/Pacific Islander (6%), and Latino (4%) children (Figure 1).
• The prevalence of asthma in each Service Planning Area (SPA) is shown in Table 1. Differences between SPAs should be interpreted with caution given the small sample size in some SPAs.
• Reported asthma prevalence did not vary by household income but was higher among children with private insurance (7%) and MediCal/Healthy Families (6%) than among those without health insurance (3%), suggesting that uninsured children may be less likely than those with insurance to have asthma diagnosed.
Impact of Asthma on Level of Physical Activity.
• Among children with asthma, 53% had limited physical activity because of their disease, including 61% of those 6 to 17 years of age.5
• The percentage of asthmatic children with limited physical activity was higher among African-Americans (63%) and Latinos (62%) than whites (36%) and Asians/Pacific Islanders (28%).6
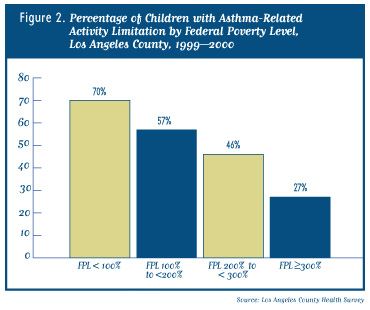
• The percentage with asthma-related activity limitation was highest among those living below 100% of the federal poverty level (70%) and lowest among those living above 300% of poverty (27%) (Figure 2).
Exposure to Environmental Tobacco Smoke.
• Overall, an estimated 8% of children in the county (or 215,000 children) were exposed to environmental tobacco smoke (ETS) in the home on a regular basis.
• The prevalence of asthma was 8% among children exposed to ETS in the home compared to 6% among children not exposed to ETS in the home (this difference was not statistically significant).
• Among children with asthma, those exposed to ETS in the home were more likely to have asthma symptoms that limited their physical activity (70%) than those not exposed to ETS (52%).
Discussion
The results of the survey indicate that approximately 6% of children in Los Angeles County have asthma, comparable to the prevalence of childhood asthma reported nationally (5.3%).3 The prevalence among African-American children in the county (16%) is markedly higher than the rate reported for African-American children nationally (6.8%). The reasons for this disparity are unclear and highlight the need for additional studies to identify the factors contributing to the higher asthma prevalence among African-American children in the county. The lower asthma prevalence observed among Latino children (4%) may reflect reduced access to health care services in this population7 and, therefore, should be viewed with caution.
The findings also indicate that among children in the county with asthma, many suffer symptoms severe enough to limit their physical activity and require emergency room or other urgent health care visits. These markers of more severe asthma were reported more frequently among African-American, Latino, and low-income children, suggesting that focused efforts are needed in the county to improve access to medical care and other support services (e.g., psychosocial support services, asthma education, and instruction on the use of inhalers and other asthma medications) for these populations. Given the potential morbidity associated with asthma and the large number of interventions available to reduce its severity, these services should be provided by, or be closely linked to, a primary health care provider who can ensure continuity of care and optimal disease management.
Public health interventions are also important for addressing the environmental factors that predispose to asthma. For example, although levels of outdoor air pollution have declined substantially in the Los Angeles basin over the past several decades, air quality remains among the poorest of any metropolitan area in the country. A number of research studies have demonstrated a link between outdoor air pollution and the severity of symptoms among those with asthma,8 suggesting that continued efforts to improve air quality in the county will reduce asthma-related morbidity and mortality. The importance of indoor air quality on both asthma incidence and severity is also well documented.9 The findings of the present survey are consistent with a number of other studies that have demonstrated an association between exposure to environmental tobacco smoke and childhood asthma,9,10 highlighting the importance of ongoing efforts to reduce smoking among adults with children. Exposures to other environmental asthma triggers (such as dust, mold, mildew, and cockroaches) can also be reduced by providing community education and addressing substandard housing conditions in the county.
The survey results are subject to at least two limitations. First, because the data are based on parent reports, children with unrecognized asthma are not included in the prevalence estimates. Studies have found that as many as 15% of children in urban settings may have asthma symptoms that are undiagnosed,11 suggesting that the results presented in this report should be viewed as minimum estimates of the burden of asthma in the county’s child population. If the assumption is made that uninsured children and those covered by MediCal or Healthy Families are just as likely to have asthma as those with private insurance, the estimated prevalence is increased to 7% (or 200,000 children). A second limitation is that the survey did not include children who are homeless or living in households without telephones, estimated to comprise at least 3% of the county’s total child population. Assuming 7% of these children also have asthma, the estimated number of children in the county with asthma is increased to 206,000.
In summary, the findings in this report indicate that childhood asthma is a significant public health problem in Los Angeles County, especially in the African-American population. The findings also suggest that many children with asthma may not be receiving adequate medical care and other support services to control their symptoms, resulting in activity limitations and the need for emergency room and other urgent care services. Efforts are needed to improve access to health care and other support services for children with asthma, and to address modifiable environmental factors that contribute to asthma-related symptoms.
Collaborative Efforts to Reduce Childhood Asthma Morbidity
The County Department of Health Services (DHS) is working with community-based agencies, private organizations, and local schools to address childhood asthma in highly impacted communities. The LAC+USC Medical Center, in conjunction with the Southern California Chapter of the Asthma and Allergy Foundation of America (AAFA SoCal) and the Los Angeles Unified School District, operates the Breathmobile®, a nationally recognized program that provides asthma screening and treatment to high-risk children in schools. The Breathmobile®, a mobile clinic, visits selected schools throughout the county on a regular basis, working with school nurses to identify and treat asthmatic children, many of whom have no regular source of health care.
DHS is also partnering with the American Lung Association on another school-based project, “Open Airways for Schools.” In this program, students with asthma participate in educational sessions to learn how to manage their disease more effectively. Parents, classmates, and school staff are also included in the educational program. The American Lung Association also offers a “Tools for Schools” program, which helps schools address indoor air quality problems that can aggravate asthma in schoolchildren.
For additional information on childhood asthma services and community resources, contact:
• Asthma and Allergy Foundation of America, Southern California Chapter: 800.624.0044; www.aafasocal.com
• American Lung Association of Los Angeles County: 323.935.5864; www.lalung.org
Acknowledgments
LA Health is a publication of the Office of Health Assessment and Epidemiology, Los Angeles County Department of Health Services, Public Health.
Series Editors: Paul Simon, MD, MPH; Cheryl Wold, MPH; Jonathan Fielding, MD, MPH; and Anna Long, PhD, MPH.
Data Analysts: Isabel Cardenas, MPH; Michele Liebowitz, MPH; Amy Lightstone, MPH, ATC; Zhiwei Waley Zeng, MD, MPH.
Administrative Support: Patricia Schenk
Special thanks to Wendy Schiffer, MSPH; Rob McConnell, MD; and Francene Lifson for their editorial assistance.
Funding for the survey was provided by the Los Angeles County Department of Health Services, the California Department of Health Services, the Los Angeles County Medicaid Demonstration Project, and the Los Angeles County Department of Public Social Services.
For more information or to obtain additional copies of this report, call 213-240-7785 or visit our web site at
www.lapublichealth.org.
1. Newacheck PW, Halfon N. Prevalence, impact, and trends in childhood disability due to asthma. Arch Pediatr Adolesc Med 2000;154:287-293.
2. California Department of Health Services, Environmental Health Investigations Branch. California County Asthma Hospitalizations Chart Book. August, 2000.
3. Centers for Disease Control and Prevention. Measuring childhood asthma prevalence before and after the 1997 redesign of the National Health Interview Survey—United States. MMWR 2000;49:908-911.
4. This definition is consistent with the uniform case definition of self-reported (or parent-reported) asthma adopted by the Council of State and Territorial Epidemiologists.
5. Children were classified as having limited physical activity if the parent reported that asthma limited the child’s activity sometimes, most of the time, or always.
6. The results for Asian/Pacific Islander children should be viewed with caution because the sample was small (n=24).
7. Los Angeles County Department of Health Services. Recent trends in health insurance coverage among Los Angeles County Children. LA Health, October, 2000.
8. McConnell R, Berhane K, Gilliland F, et al. Air pollution and bronchitic symptoms in Southern California children with asthma. Environ Health Perspect 1999;107:757-760.
9. Weiss KB, Gergen PJ, Wagener DK. Breathing better or wheezing worse? The changing epidemiology of asthma morbidity and mortality. Annu Rev Publ Health 1993;14:491-513.
10. Weitzman M, Gortmaker S, Walker DK, Sobol A. Maternal smoking and childhood asthma. Pediatrics 1990;85:505-511.
11. Joseph CLM, Foxman B, Leickly FE, Peterson E, Ownby D. Prevalence of possible undiagnosed asthma and associated morbidity among urban schoolchildren. J Pediatr
1996;129:735-742.